Frequently Asked Questions ( FAQ's)
What is infertility?
Infertility is commonly defined as inability to conceive within 12 months of regular natural unprotected sex.
How common is infertility?
Infertility is a common disorder. About 10-15% of world’s population suffer from it.
What are the main causes of infertility?
The causes are distributed among men (30%), women (30%), both (20%) or even – in rare cases – the cause can be inexplicable (20 %).
In 80% of cases, female infertility is due to:
- Fallopian tubes: when they have some type of injury.
- Endometriosis: when a part of the uterine tissue goes outside the uterus.
- Ovulatory dysfunction:
- Diminished Ovarian reserve due to advancing age. From 35 years, the reproductive potential decreases and by 40, the possibility of pregnancy is 10%
- Other risk factors:
- Sexually transmitted diseases
- Chronic diseases (diabetes, cancer, thyroid, depression)
- Myomas
- Drugs such as antidepressants
In men, the main causes are usually:
- Alterations in the genital tract (which may make it impossible to deposit the semen deep in the vagina during intercourse).
- Erection problems.
- Very pronounced curvature of the penis or great decrease in it.
- Alterations in the production of semen (decrease in quality and quantity).
- Extreme obesity.
Is infertility becoming more common nowadays?
Statistically, infertility has remained at the same level through the years. What has become common is the level of fertility treatments that have become more affordable and more successful than the past. So, the couple resigned to lack of children, now hope and get treated for the causes of infertility.
What type of fertility treatments do you offer?
At PSFC, we offer diagnostic tests and treatments to both men and women and the treatment is holistic. We start with Fertility Assessment for the couple, tell them about Fertility Wellness, explore treatment through simple medication and inexpensive Artificial insemination methods. We extend the treatment to IVF, ICSI and offer Donor programs to couples who do not conceive still. We also do invasive surgeries for both males and females like TESE, Laparoscopy, embryo biopsy, PGT etc.. This places us at the highest level of quality to achieve the best pregnancy rates.
Are the fertility treatments guaranteed to achieve a pregnancy?
No guarantee is ever possible by any Fertility Centre in the world. However, the probability of success (of conception) can be improved through various treatments and surgical interventions on both men and women. In infertile couples, donor program (egg, sperm or embryo) greatly enhances the chance of conception. At PSFC, 72 out of 100 infertile couple got treated and conceived.
How does Human Reproduction System work?
The human reproduction system consists of the Male and the Female Anatomy.
The male reproductive system consists of two major parts: the testes, where sperm are produced, and the penis. The testes are carried in an external pouch known as the scrotum, where they normally remain slightly cooler than body temperature to facilitate sperm production.
The major internal organs of the female reproductive system include the vagina and uterus — which act as the receptacle for semen — and the ovaries, which produce the female’s ova. The vagina is attached to the uterus through the cervix, while the fallopian tubes connect the uterus to the ovaries. In response to hormonal changes, one ovum, or egg — or more in the case of multiple births — is released and sent down the fallopian tube during ovulation. If not fertilized, this egg is eliminated during menstruation.
Fertilization occurs if a sperm enters the fallopian tube and burrows into the egg. While the fertilization usually occurs in the oviducts, it can also happen in the uterus itself. The egg then becomes implanted in the lining of the uterus, where it begins the processes of embryogenesis (in which the embryo forms) and morphogenesis (in which the fetus begins to take shape). When the fetus is mature enough to survive outside of the womb, the cervix dilates, and contractions of the uterus propel it through the birth canal.
All of our initial testing came back normal; why am i not getting pregnant?
The initial testing is useful in detecting large problems such as low sperm counts or blocked fallopian tubes. Approximately 20-25% of patients presenting with infertility will have normal testing (called “unexplained infertility”). This may be at least partly explained by an age-related decline in fertility. Often times we are able to obtain further information as to why you have not gotten pregnant through monitoring and may be able to help overcome this underlying infertility with treatment.
Fertility treatments increase the possibility of having twins, triplets or more babies
Assisted reproduction in not synonym for multiple pregnancies. Many are the studies which currently are aimed at reducing these types of pregnancies and avoid certain complications during pregnancy. The selection of the best embryos is key to transfer a lesser number. This way, egg stimulation, the embryo transfers and the culture techniques in the laboratory have been optimized. The latter helps embryos reach blastocyst stage. Following this procedure, we increase the chances of pregnancy with the transfer of one embryo and hence reduce the chances of a multiple pregnancy. These are some of the most common myths on Assisted Reproduction. If you have any doubts, you can always contact a professional in the field. At PSFC we will be delighted to help out!
What causes infertility?
In addition to poor quality eggs or blocked tubes, endometriosis is also attributed to causing infertility in females. Poor sperm quality or count is usually the cause of male infertility.
When should one get treatment and get evaluated for infertility?
Women are evaluated for infertility on the second day of menstruation, and semen analysis is done after 3-5 days of sexual abstinence. Various tests like hormone levels, pelvic exams, ultrasonography, semen analysis, and infectious diseases can be done during this period. If required, the inside of the uterus is best examined after menstruation. Doctors can decide the best form of treatment after consulting the results of these tests.
Are there specific postures which are in favor of a gestation?
There are no scientific studies which demonstrate that specific postures improve the chances of a pregnancy, as there are no studies that mention the benefits of keeping your legs up after intercourse to help getting pregnant. Spermatozoids have their own mobility which is independent to gravity. What is truly important is the concentration of spermatozoids with progressive mobility in the ejaculation, not the force of gravity.
What is meant by fertility assessment?
A fertility assessment is a series of tests, including an AMH blood test and an antral follicle count, used to measure your egg count and assess other potential barriers to fertility. Together with your age and medical history, these tests give a doctor a clear picture of your fertility health and how successful egg freezing may be for you.
While your OB/GYN or at-home testing kits may be able to perform some of these tests, we strongly recommend doing this testing with an experienced fertility provider who will be best able to interpret the results. Contact us at PSFC to schedule Fertility Assessment. Call 91500 91800
Does age influence pregnancy?
Age is the most crucial factor in relation with the ovarian reserve and fertility.
The reason being that at birth, women already have all the eggs available to them and, throughout their lives, these eggs decrease due to a destruction process, called apoptosis.
Even though two women of the same age can have better or worse ovarian reserves, the amount and quality of the eggs always decrease with age.
What are treatment options for secondary infertility?
First, we do tests to find the cause(s) – including diminished ovarian reserve (low egg supply), hormonal issues, blocked tubes, polyps or fibroids inside the uterus, or sperm problems. Treatment depends on the results but may include fertility tablets like Clomid or letrozole with Intrauterine Inseminations (IUI) injectable medicines and IUI In Vitro Fertilization (IVF)” egg donation or embryo donation.
Is IVF covered under insurance in India?
In India, no insurance company covers for IVF , reason being health insurance covers for illness and diseases majorly which requires hospitalization. IVF – which is a treatment to get pregnant and pregnancy related conditions are not termed as illness and hence not covered in mediclaim insurance. Maternity is covered in Corporate health policy but IVF is mostly not covered.
But currently few companies are giving Infertility and maternity benefit cover :
- New India – Mediclaim Policy: New India Assurance has announced a mediclaim cover which will cover the cost of infertility too, but the individual policy terms have to be read carefully before binding of risk.
- Bhartiya Mahila bank started a policy covering IVF but after it was merged with SBI the policy got discontinued.
- Star Health Insurance — Family Health Optima
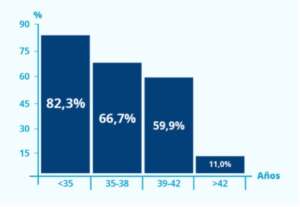
Does age influence fertility treatments?
As the woman’s age increases, the chance of success through conventional methods decreases. Clinical interventional methods such as IVF and ICSI are the recommended treatments.
The rates for pregnancy with in vitro fertilisation depend on the patient’s age. We can see on this graph the rates for pregnancy by age groups after the transfer of fresh and frozen embryos from the same cycle.
At what age do women stop being able to have children?
On average it’s in the 40’s, and fertility for most women is very low at 45 and older with their own eggs. There are many individual factors however – we see women in their 20’s who can’t conceive naturally, and there are healthy pregnancies in 47 year olds, and everything in between. Using egg donation there may be no biological upper limit but risks are higher in the 50’s: women 55 and older should not try to conceive.
At what age should I begin to be concerned about infertility if I don’t want a baby yet?
If you’re asking, you’re already beginning to be concerned. In general, peak fertility for women is in the 18-30 age range, and fertility decreases in your 30’s and 40’s. All women are different – there is no age where everyone can get pregnant or no-one can get pregnant; having said that pregnancy is much less common at 45 years and older. On average, your fertility goes down every year from age 40 to 45.
I would start to be more seriously concerned as you get closer to the 38-40 age range, but if you have a fertility issue at 38 it would be better to find out sooner rather than later. There is a lot of individual variation in ovarian reserve or egg supply (the number and quality of eggs that a woman has left) at any age, so there are 35 year olds with good egg supply and 35 year olds with diminished ovarian reserve.
If you’re aware of your fertility but don’t want a baby yet it wouldn’t be unreasonable to do some basic tests to get an idea of how healthy your ovaries look at 35. These would be an ultrasound scan of your ovaries, looking at the size of each ovary and the number of egg-containing follicles on each side or Antral Follicle Count, and blood tests on Day 2 or 3 of your cycle for estradiol, Follicle Stimulating Hormone or FSH, and Antimullerian Hormone or AMH. Day 1 is the first day of your period. If you’re on hormonal birth control such as pills, NuvaRing, Mirena or Implanon we would skip the estradiol and FSH tests. A fertility clinic (Reproductive Endocrinology and Infertility or REI practice) can perform these tests and interpret the results.
If the results look good you can relax and wait a couple of years longer before trying. If there’s a problem with low ovarian reserve, options include freezing your eggs if you’re single or not in a long-term relationship, or freezing embryos for later use if you have a partner or wish to use donor sperm but aren’t ready to get pregnant now. You could also decide to pursue fertility treatment sooner based on the results.
At 40, can I still get pregnant?
Being over 40 years old is not an obstacle to be a mother, but the quality of the eggs is worse and that causes fertility decreases. In addition, from the age of 40, the risk of complications is greater. However, both things are not sufficient reason to give up being a mother.
Unfortunately, there is a biological clock, and although it starts to tick louder at different times for different people it is very probable that you are going to have some issues over the age of 40. That being said, the only way to find out exactly what your chances of success will be with your own eggs is to have a series of fertility investigations carried out. We will be able to give you a better understanding of your own fertility after that, and then help you decide between the idea of either using your own eggs or those of an egg donor.
What risks are we talking about specifically?
Risks for the woman
When this age is reached, the risk of suffering diseases which are associated to this age, is greater, and therefore pregnancy can be considered a risk situation. In addition, the possibility of suffering gestational diabetes is greater, and deliveries can be prolonged in the case of new mothers.
Risks for the baby
For the baby, it carries a higher risk of chromosome disease (such as Down syndrome) or mild heart disease. It also increases the possibility of miscarriage or premature delivery.
It’s not all bad news
The good news is that the number of women who decide to have children after turning 40 is increasing, so the control of the risks during pregnancy and the good health results of the mother and child, as well.
In addition, thanks to scientific advances in fertility, it can be said that the batteries of the biological clock are day by day more durable. If you are over 40 and want to be a mother, do not focus on thinking “I already missed the boat”. Find professionals who advise and accompany you during the experience and you will reduce risks to the maxim.
If you want more information, PSFC has the perfect team to advise you. Send us an email to enquiry@psfc.in or call at 91500 91800. We are waiting for you!
Pre-menopause. Can I be a mum?
Pre-Menopause is an ilness which affects more and more women and it’s diagnosis can worry them as the tendency is to think they can never have children. However, it’s possible to be a mother thanks to ART.
What is pre-menopause?
Pre-menopause ocurrs when a woman loses her ovarian function, diminishing the flow of estrogen. The age of menopause comes determined by the particular ovarian reserve of each woman at birth, and by the rhythm at which those eggs are used up during the menstrual cycle. Generally, it ocurrs between the age of 45 and 55, but if it’s before the age of 40, it’s pre-menopause.
The reasons why menopause occurs are various. It can be due to genetic factors, which in many cases means that women with menopause have a family history of early menopause. It can also occur after carrying out oncologic treatments such as chemotherapy or radiotherapy, due to a premature ovarian failure or to an ovarian surgical intervention
What are the pre-menopause symptoms?
Menopause implies the loss of fertility and can carry negative physical and psycological conseuqences. The first sign of pre-menopause is irregular periods that can go on for a few months. Furthermore, there can be vaginal driness, changes in mood, depression, lack of libido, hot flushes and difficulty to fall asleep.
Is it impossible to have a baby once menopause has finished?
Menopause really means that your periods have stopped forever, but in practice we consider it menopause after a year with no periods in women in the typical age range for menopause (average age is 51). There is a very very small chance of releasing an egg and getting pregnant after ‘natural’ menopause with one year of no periods. This chance is much higher in women who go through ‘premature menopause’ at a young age, which is more correctly known as Primary Ovarian Insufficiency or POI, and can happen in the 30’s or even 20’s. Obviously surgical menopause, after both ovaries have been removed, has very little chance of pregnancy at any age, though sometimes part of an ovary is left behind after surgery.
So assuming you are around 50 and have had no periods for a year, the chances are very slim of getting pregnant naturally – close to zero but not impossible. Egg donation is very successful (75% to 80% success rates and higher) for women with POI or menopause of any age who want to get pregnant, but most clinics have a maximum age for treatment. If there is no disease of the uterus success rates are as high as for younger women, but there can be more pregnancy complications and a higher risk of C/section. Some women have medical problems like kidney disease which may make pregnancy inadvisable. Talk to your Ob/Gyn or see a Fertility MD if you do want to have a baby.
Can I get pregnant if I am a single woman?
We do not make any judgments against single women seeking treatment and all infertility investigations are going to be carried out the same as they would be for the female half of a couple. The only difference is that you will need to use sperm from a donor, but there are plenty of donor sperm banks that have a wide range of different donors to choose from. We are able to use sperm from a number of these different banks and we will advise you the best way of proceed with that selection.
Can I get pregnant after my partner had a vasectomy?
In the case of a vasectomy, there are a few options open to you to try and conceive. Potentially the simplest treatment is to use donor sperm. This is not always an option that some couples would like to take, and there are ways to attempt to obtain your partners sperm after the vasectomy. The first is to actually reverse the vasectomy, a surgical procedure that is carried out by a urologist. A potential benefit of this is that if the reversal is successful, you may not need any more intervention to achieve a pregnancy. The problem though is that there are often a lot of other issues that come with that surgery that dictates the need for further treatment such as IUI or even IVF anyway. Another option is to attempt surgical sperm retrieval, again in a urology office. This will, in most cases, also require the woman to undergo an IVF cycle, but depending on the length of time since the vasectomy was originally carried out it may be more appropriate.
Can I get pregnant if I am in a same sex couple?
As far as same sex couples go there are several different ways that treatment can be carried out.
When we are talking about treating a female couple then we can either do an intrauterine insemination with donor sperm or we can move to IVF if needed, again with the use of donor sperm. If the treatment is going to be IVF, then it is possible to use the eggs of one of the couple and then after insemination with donor sperm, the other woman could have the embryos transferred into her uterus. In this situation it will potentially allow them both to feel more connected to the child.
In the case of a male couple, it is going to be a little more complicated as there is going to need to be an egg donor and a surrogate to carry the pregnancy. This could potentially be in the form of traditional surrogacy when an IUI with the sperm of either of the guys is used, or more commonly when an egg donor undertakes an IVF cycle, and the resultant embryos are transferred into a separate surrogate.
In any of the above-mentioned situations there will need to be legal documents drawn up and we can point you towards appropriately informed experts.
Can I check to see if I am OK to wait a few years before having kids?
If you want to have fertility testing but are not ready to start a family yet then we can help. We can now offer women an inexpensive way to find out what their fertility potential is. Through a couple hormonal tests, and a simple ultrasound we can now create a customized fertility assessment. Learn more about our Fertility Assessment program and see if it makes sense for you.
Do I need a referral from my Ob/gyn or Primary Care MD to see you?
ORH does not require a referral, but your insurance company may require that you have one. Check with your insurance plan if you need a referral or if you must register with them to get fertility coverage. If you are referred by a physician or other health professional, please let us know. It is helpful to request records of your previous testing and treatment so that we can review them. Many of our patients are referred by friends, coworkers, or family members, including former patients of ours who have been successful.
What is the difference between a Fertility specialist and seeing my Obs/Gyn?
Reproductive Endocrinology and Infertility or REI MDs are sub-specialists: we train in Obstetrics and Gynecology (OB/Gyn) then do advanced study of male & female hormonal conditions (endocrinology) and infertility testing and treatment including IVF. REI should be board-certified, except for a few older docs. Ob/Gyn MDs offer prenatal care, delivery, gynecologic care & surgery. Fertility specialists can help you get pregnant, including women with recurrent miscarriage, and look after you in early pregnancy, before transferring your care to an Ob/Gyn when you’re ready to graduate from our program!
How long should we try before seeing a Fertility doctor?
You may consult a fertility physician (Reproductive Endocrinologist or REI) any time if you have difficulty conceiving. You can try for up to a year if you are 34 or under, or for up to 6 months if you are 35-39. See a REI right away if you are 40 or over, if you have irregular cycles, if you have had a previous ectopic pregnancy, chlamydia, or Pelvic Inflammatory Disease, if you have had endometriosis or ovarian surgery, or if your partner has known sperm issues.
Can a woman who enters menopause prematurely have children?
Yes, it is possible. A woman who has entered menopause means that her ovulation (ability to produce own eggs) has stopped but that does not prevent donor eggs to be inseminated with her partner’s sperm as is done in a regular IVF procedure.
How common is infertility?
According to the World Health Organization (WHO), about 10-15% of couples struggle with infertility problems. That’s approximately 70-80 million people across the world, so you’re not alone if you face these challenges.
Is infertility primarily a female problem?
While commonly asked by couples anticipating fertility services, the answer is a resounding “No”. In fact, infertility in women and men is almost identical, attributed to females 1/3 of the time, males 1/3 of the time, and unidentifiable the last ⅓ of time.
Is infertility hereditary?
Genetics can be a factor in determining fertility. There are many different conditions that can be passed from mother to daughter, such as endometriosis (which affects 10% of women). For males, DNA abnormalities of the Y chromosome can lead to problems with infertility.
What causes infertility?
Couples seeking fertility services often ask, “Why are we infertile?”. At PSFC, we break it down to male and female infertility. Common female infertility is caused by anatomical abnormalities and problems with ovaries or egg quality. Male infertility includes issues related to quantity and quality of sperm production, immunological disorders, and anatomical issues.
What treatment options are available for people struggling with infertility?
There are several options, though your doctor will need to advise on what most increases your odds of success. Some people need more intervention than others. Some female patients have success conceiving with oral fertility hormones such as clomiphene citrate. Some will need injectable ones such as gonadotropin. The treatment of male infertility on the other hand, often requires IVF with intracytoplasmic sperm injection (ICSI).
Does infertility treatment work?
Yes! This is one of the most popular in vitro fertilization (IVF) frequently asked questions. The success of treatment has a direct correlation with the woman’s age. The younger the better! Overall, 70-80% of women under the age of 40 should expect a successful outcome. If you’re over 40, treatments can still be effective. However, the average success rates decrease once beyond this point in life. Please note that treatment outcomes can vary widely from individual to individual.
What influences the success of infertility treatment?
The most important factor for a woman is her age. As her age increases, especially after 40, fecundity decreases, and her chances of conceiving are diminished. Of course, if her partner also has infertility problems, such as a low sperm count, the probability of infertility also increases. For men considering infertility treatment, low sperm motility or other infertility can be avoided through ICSI, PGD/PGS, and more.
Are there health risks for children born through infertility treatment?
Of all of the in vitro fertilization (IVF) frequently asked questions we get from hopeful parents, the health of their children is often at the top of the list. There are conflicting reports that suggest a slight increase in the congenital anomalies with IVF. you should speak with a medical expert before making any decisions. If you want to learn more about IVF, browse our website or for specific questions, or simply contact PSFC today.
How much does fertility treatment cost?
Depending on the services you require, infertility treatment can range from $200 to many thousands of dollars. Everyone faces different infertility challenges, so diagnosing and treating patients is highly variable. However, for individuals struggling with finances, we offer payment plans and financial support throughout this process. To find out more about fertility treatment expenses, visit PSFC
Will my insurance cover infertility treatments?
It depends. Like above, because everyone faces different infertility challenges and requires different treatments, you may receive none, partial, or full coverage. To determine what your insurance will cover for infertility treatment, contact us with a picture of your insurance card (front and back) and your date of birth. We would be happy to run an insurance authorization check to let you know what’s covered. Additionally, contacting your insurance provider and employer will be important to determining what coverage you receive.
What is the most effective procedure and medication for couples with unexplained infertility?
After fertility testing, we rarely see ‘unexplained infertility’. We used to think 15-20% of infertility was ‘unexplained’ (with regular cycles, open tubes, and good sperm) – with modern testing it’s under 1%. Ovarian reserve testing (ultrasound for ovarian volumes and antral follicle count, Antimullerian Hormone or AMH and the Clomid Challenge test) ‘explains’ a lot but there are other possible factors. See a board-certified Reproductive Endocrinology and Infertility or REI specialist for more detailed testing and to give you treatment choices: inseminations (IUI) combined with medications to increase the number of eggs IVF can be appropriate depending on your case.
How long after conception does a person usually find out that they are pregnant?
Roughly two weeks after conception, or about 15 days after a positive ovulation test. If your pregnancy hormone levels are high enough, home pregnancy tests may turn positive a few days before the date of your ‘missed period’. Blood pregnancy tests are more sensitive.
What are the first steps in an infertility evaluation?
See a Reproductive Endocrinology and Infertility or REI MD, who will review your medical history and your partner’s history, examine you, and recommend appropriate fertility tests for both of you. These may include blood work to check your ovarian reserve (egg numbers and quality) and to check for hormonal problems, an ultrasound scan of your uterus and ovaries, a Hysterosalpingogram (HSG) to check your tubes, and a Semen Analysis for him.
What can I do if we want to have twins?
Be careful what you wish for … twins are more high risk than a single baby, although most twins do fine with good OB and neonatal care, some twins have long-term problems, some are premature and some don’t even make it to viability and are born before 24 weeks. The risk of cerebral palsy, a serious birth defect, is 4 – 5 times higher in twins compared to a single baby. You have a higher chance of pregnancy complications including serous ones like preeclampsia or placental abruption, a higher risk of C/Section, and even a very slight increase in divorce rate.
I know the baby photographers all love to show pictures of cute twins all dressed up … the kids with cerebral palsy are generally not shown on the front cover of a magazine.
Couples who need treatment for infertility, from simple treatments like Clomid to advanced treatments such as In Vitro Fertilization (IVF), often have an increased risk of twins if more than one egg is released with fertility medications, or if more than one embryo is replaced into a woman’s uterus after IVF.
If we’re treating couples for infertility who can’t get pregnant on their own twins may be an acceptable risk of the treatment. Many couples tell me they want twins – they have been trying for a baby for one or many years, and many couples want two babies total and would love to have twins and ‘be done’. We do our best to avoid triplets or more, though. In this case the risk of twins is justified by the benefit of treatment of their infertility.
If you don’t have any problems getting pregnant your natural chance of twins is about 1%. I don’t recommend going to an Ob/Gyn or Fertility MD just because you want twins (wanting twins for social reasons””) – if you end up with complications to you or the babies” would it be worthwhile compared with just having two more kids separately? I would not recommend “getting fixed” in your early 20’s until you are 100% sure that you’re done either we have great birth control options like the Mirena IUD which is about as effective as having your tubes tied but reversible if you have one more child and then want another one later.
What is the best way to see if we can get pregnant?
About 85% of couples get pregnant after a year of trying. It could still happen ‘naturally’ (at two years it’s over 90%) but if you have been trying for more than one year or more (under 35 years of age), 6 months or more (36-40 years of age) or if you are over 40 years of age this is a good time to see a Fertility specialist (Reproductive Endocrinology/Infertility or REI) to find out why your partner is not getting pregnant and to help you to get to that first child.
REI physicians train in Ob/Gyn before specializing in fertility medicine. They can do tests to check the number of eggs left in the female partner’s ovaries (ovarian reserve) which can go down as women get older. She should also be checked for hormonal problems which can stop her from getting pregnant including thyroid problems or polycystic ovarian syndrome (PCOS), and the MD will check her uterus for fibroids or polyps and perform a hysterosalpingogram or HSG test to make sure that her fallopian tubes are both open and look normal.
It takes two to get pregnant of course, and the man has a sperm problem in 40-50% of couples trying to conceive, so you will need a semen analysis (sperm test). If there is a sperm issue, it may be the only reason that the female partner is not pregnant yet, or a contributing factor along with problems on the female side. Most REI docs like to see you both partners as a couple, but it is not mandatory that you come to the first visit.
After these tests there are specific treatments for improving fertility depending on the cause(s) we find, such as Clomid can help her ovulate (release an egg) or release more than one egg in a month. Clomid can be combined with Intrauterine Inseminations (IUI) where the sperm is washed and placed inside her uterus. Some couples may need more intensive treatment such as In Vitro Fertilization (IVF).
In short, see a specialist for testing and to come up with an individualized treatment plan to help your wife get pregnant. Lifestyle changes may help if needed as well – quit smoking, avoid heavy drinking and drug, and aim for a normal weight applies to both of you.
It is now possible for women interested in knowing their reproductive potential to obtain a detailed fertility assessment. Our new Fertility Snapshot program lets women know just how easily they will be able to get pregnant in the next couple of years without going through costly testing.
Are there any services available to help me (and my partner if applicable) through this very stressful fertility journey?
Yes, there are many services available. Through PSFC we can arrange psychologist support who offer individual and couples counseling, acupuncture, The Mind Body Program and nutritional counseling with a registered dietician. Also we have an in-house psychologist staff at PSFC who can counsel you.
What is a Certified Clean Room for Ultra IVF?
In addition to undergoing the genetic screening process, part of our Ultra IVF is the fact that we determine, or measure, all of the components that could impact the embryo environment. These components consist of the air quality. We have installed in our labs several hepa air filters, which have allowed us to be certified as a “Clean Room.”
What a Clean room means is that there’s not very much dust, dirt or contamination in the air, very much like what is done when people are working on a microchip. You cannot let dust land on a microchip because then it will cause it to short circuit. Same thing with an embryo, an embryo is microscopic and any piece, no matter how small, of dust or contamination can cause that embryo not to progress.
How does a Certified Clean room benefit patients?
Providing a Certified Clean Room is a very expensive process. The level of filtration that you need in order to reach those standards is very expensive. We have provided that because of the fact that I care about whether or not the patient gets pregnant. I will do everything within my power to provide the right environment for that embryo to succeed and so I believe heavily in anything that I know that contributes to the embryo’s progression. I want those factors controlled and that’s what we do in PSFC. We control the temperature, the pH of the environment. All of these things are tightly controlled so that the embryo goes through a lot less fluctuation.
I have also actually provided more incubators in the lab than what is needed to carry out the number of cycles that we are doing because to me, the individual incubation plays a huge role in whether or not the embryo will be successful. The more the door is open to the embryo’s, the more fluctuation they undergo when they are trying to progress and develop into what’s going to be a baby someday so therefore, we like to limit the amount of times we need to open and close the doors to the incubator and by having individual incubation units, we can do that here at Red Rock Fertility Center. We’ve seen that not only are the success rates high, but the babies are smart, beautiful and everything you’d love them to be.
How Air quality improves your IVF success ?
The difference between a certified clean room and right now we’re at a class 1000 and regular room air is that a certified clean room is 1000 times more pure air than the regular environment. If IVF were conducted in a regular room like this office, it is 1000 times more likely that a speck of dust would land in the dish of an embryo here than in the IVF lab.
Read More FAQ’s on : MALE FERTILITY | FEMALE FERTILITY | FALLOPIAN TUBE | TUBAL LIGATION | PCOS | FERTILITY ON NATURAL WELLNESS | IUI | IVF & ICSI | PCD | DONOR PROGRAM | FERTILITY MEDICATION | FERTILITY PREVENTION | EGG FREEZING | EMBRYO FREEZING